Module Six: Disability-Informed Genetic Counseling in Practice
Introduction
This final module brings together everything covered in the first five modules including language, communication, social context, lived experience, family dynamics and rights-based frameworks, and it applies those concepts directly to genetic counseling practice. Rather than viewing disability as a single topic addressed at one point in a session, this module emphasizes that disability-informed care is a thread woven through every stage of the genetic counseling process.
Through case-based reflection and video narratives from individuals with disabilities and their families, learners will examine how small, intentional shifts in preparation, communication, and advocacy can meaningfully improve trust, autonomy, and equity in genetic counseling encounters.
6.1 As a Student
Genetic counseling students and trainees are still building clinical skills and professional identity. This stage of training is an important opportunity to develop disability-informed habits early, before patterns of practice are established. While students may not control clinic systems, they do have control over how they prepare, listen, and engage with learning.
Disability-informed care does not require knowing everything—it requires curiosity, humility, and a willingness to learn. Recognizing gaps in training is not a failure, but an opportunity to seek out resources, ask questions, and grow as a more inclusive provider.
Video: Gaps in Deaf Education Among Health Care Providers
This video highlights how limited disability and Deaf education in healthcare training can lead to communication breakdowns and inequitable care, underscoring the importance of intentional preparation and ongoing learning.
Video: Learning From Deaf Communities to Improve Provider Education
This clip emphasizes the importance of community-informed, lived-experience–centered education for healthcare providers and encourages approaches rooted in humility, listening, and partnership.
6.2 Case Preparation
Disability-informed care begins before the patient enters the room.
Video: What Families Carry into the Room
This clip highlights the often invisible emotional and logistical “extra packages” that individuals and families bring with them into healthcare encounters. It encourages genetic counselors to approach case preparation with awareness and an understanding of the unseen work patients and families are already doing.
Case preparation should include reviewing records with an awareness of how disability has historically been medicalized, framed, or restricted to diagnoses. Genetic counselors should note how language is used in prior documentation and be prepared to reframe terminology during the session if it is outdated, stigmatizing, or deficit focused.
Preparation also includes anticipating access needs. Reviewing intake forms for preferred communication methods, accommodations, or support persons allows counselors to proactively reduce barriers rather than reacting during the session. This step reflects lessons from earlier modules emphasizing accessibility, respect for autonomy, and the impact of systemic barriers on health care experiences.
🔧Tool for Genetic Counselors
This disability-informed case preparation checklist is a pre-session planning tool that genetic counselors can use during case preparation to intentionally evaluate accessibility, communication needs, documentation, and family context, ensuring more inclusive and patient-centered care before the encounter even begins.
🔧Tool for Genetic Counselors
This patient intake form is designed to be sent to a patient before their appointment (or at check-in) to help the genetic counselor understand patient communication preferences, accessibility needs, support system, and personal goals, so they can provide care that is individualized and centered on what matters most to you.
🔧Tool for Genetic Counselors
This telehealth accessibility form is designed to be completed before a patient’s virtual appointment to help the genetic counselor understand the patient’s technology access, communication preferences, and support needs, allowing them to tailor the telehealth visit to be comfortable, accessible, and responsive to individual needs.
Click to View:
6.3 Contracting
Contracting is a critical opportunity to model disability-informed communication. Counselors should explicitly invite patients to share preferences about identity, communication style, format of information, involvement of caregivers, and decision-making roles. Rather than assuming capacity or dependence, contracting reinforces that the patient is the primary participant in care.
Counselors should also normalize accommodations during contracting. Framing accommodations as standard practice rather than special requests reduces stigma and aligns with the social model of disability introduced earlier in the course. This step helps establish mutual respect and psychological safety early in the session.
Video: Why Preferences Matter in Care
This clip emphasizes the importance of asking individuals about their preferences rather than making assumptions. It illustrates how honoring preferences supports autonomy, trust, and more equitable genetic counseling encounters.
How to ask about accommodations (If needs are unknown)
🔧Tool for Genetic Counselors
This disability-inclusive accommodations guide is a quick reference resource that provides examples of potential accommodations across multiple domains — such as physical, sensory, communication and cognitive support — to help genetic counselors and health care teams offer flexible, individualized and accessible care based on each patient’s needs and preferences.
Opening the conversation
“We want to make sure this visit works well for you.”
Normalize accommodations
“We routinely ask everyone about accessibility and communication preferences, because people have different needs.”
Offer examples without assumptions
“Some people prefer more time, written summaries, breaks, or different ways of communicating. Others don’t need anything at all.”
Invite patient-led preferences
“Is there anything we can adjust today to make this appointment more comfortable or accessible for you?”
Provide permission to speak up later
“If something comes up during the visit or stops working for you, please let me know — we can adjust as we go.”
If a support person is present
“I’ll direct questions to you, and you can let me know how you’d like others involved.”
6.4 Medical History
When collecting medical history, genetic counselors should remain aware that disability is often documented through a deficit lens. A disability-informed approach balances clinical relevance with respect for how individuals understand their own bodies and experiences.
Open-ended questions allow patients to describe their health, functioning, and challenges in their own words. Counselors should avoid framing disability as synonymous with suffering or limitation, instead exploring what aspects of health are most relevant to the patient’s goals and concerns. Extra time, visual supports, or alternative phrasing may be helpful, particularly for individuals with cognitive, communication, or neurodivergent disabilities. This approach reflects themes from the lived experience and communication modules, reinforcing that accurate information often emerges when patients feel respected and unhurried.
Examples of Open-Ended Questions During Medical Intake
Can you tell me a little bit about your health history in your own words?
How do you usually describe your condition or diagnosis?
How does this condition show up for you day to day?
What treatments, therapies, or supports are you currently using?
Do you work with any specialist or allied health providers?
Are you currently taking any medication or using medical supports?
Have things stayed consistent, or changed overtime?

Reflection Prompt for Learners:
Case Example: You are meeting with a patient referred for genetic counseling due to a longstanding neurological condition. Prior clinic notes focus heavily on diagnostic labels and symptom severity, and much of the medical history is framed in terms of functional limitations. During the appointment, the patient answers questions politely but briefly and does not expand unless prompted. You notice that most of the information being gathered centers on what the patient “cannot do” rather than how they experience their health in daily life.
Describe one specific change you could make in your medical history intake to center patient expertise and daily life. How might this change affect trust or understanding during the session?
6.5 Family History
Family history collection offers insight not only into genetics, but also into family dynamics, beliefs about disability, and intergenerational experiences. Disability-informed family history intake involves being attentive to how families talk about disability, adaptation, care roles, and resilience.
Counselors should be mindful not to pathologize disability-related traits that families may view as identity, heritage, or difference rather than deficit. When discussing recurrence risks or inherited conditions, language should remain neutral and values-based, allowing families to interpret meaning through their own cultural and personal lenses.
Disability-informed language when discussing family history and recurrence risk
Case Example: A prenatal genetic counselor is meeting with a family in which multiple relatives are autistic, and the couple is currently pregnant. The patient does not view autism as something to be fixed, but as an important part of family identity.
What to Avoid: Pathologizing/Deficit-Focused Approach
“Since autism runs in your family, there is an increased risk that future children could also be affected. Many families find this challenging, so we will often explore testing options to better understand or potentially avoid this outcome.”
Why this can be problematic:
- Frames autism, primarily as a negative outcome.
- Assume shared family values about prevention.
- Implies burden without asking the families’ perspective.
Best Practice: Disability-Informed, Values-based Approach
- “Based on what you’ve shared about your family, it sounds like autism is something that shows up across generations in different ways. Genetically, that does mean there may be an increased chance for future children to share similar traits.”
- “Different families feel very different about what that means. Some see it as a part of their identity or family history, while others want more information for planning or support.”
- “Before we talk about testing or recurrent numbers, can you share how you think about this in your family?”
Why this works:
- Uses neutral, descriptive language.
- Separates genetic probability from value judgment.
- Invites the family to define meaning.
- Respects cultural and personal perspectives.
This step builds directly on the family dynamics module, reinforcing the importance of honoring diverse family systems and perspectives.
Reflection Prompt for Learners:
How can you balance discussing genetic patterns and recurrence risk while allowing families to define what those patterns mean for them emotionally, culturally, or practically?
6.6 Genetics Education & Testing
Providing genetics education and discussing testing options requires careful attention to framing. Disability-informed counseling emphasizes neutrality, balanced information, and respect for reproductive and personal autonomy.
Counselors should clearly separate information from assumptions about quality of life, ensuring that testing is not implicitly positioned as a way to “prevent” or “avoid” disability unless the patient frames it that way. Visual aids, plain language explanations, and check-ins for understanding can improve accessibility for many learners, not only those with identified disabilities.
🔧Tool for Genetic Counselors
This plain language examples guide provides genetic counselors with practical, patient-centered dialogue examples to help explain complex genetic concepts — such as testing, risk, and results — in a clear, respectful, and non-directive way that supports understanding and shared decision-making.

Examples of plain language explanations
Explaining What Genes Are
- Instead of: “Genes are segments of DNA that encode proteins.”
- Plain-language dialogue: “Genes are pages of instructions in our bodies that help guide how things grow, develop, and function.”
Explaining genetic conditions
- Instead of: “This condition is caused by a pathogenic variant.”
- Plain language dialogue: “This happens because one of the bodies instruction pages has a misspelling in it. That misspelling affects how the body does a specific job.”
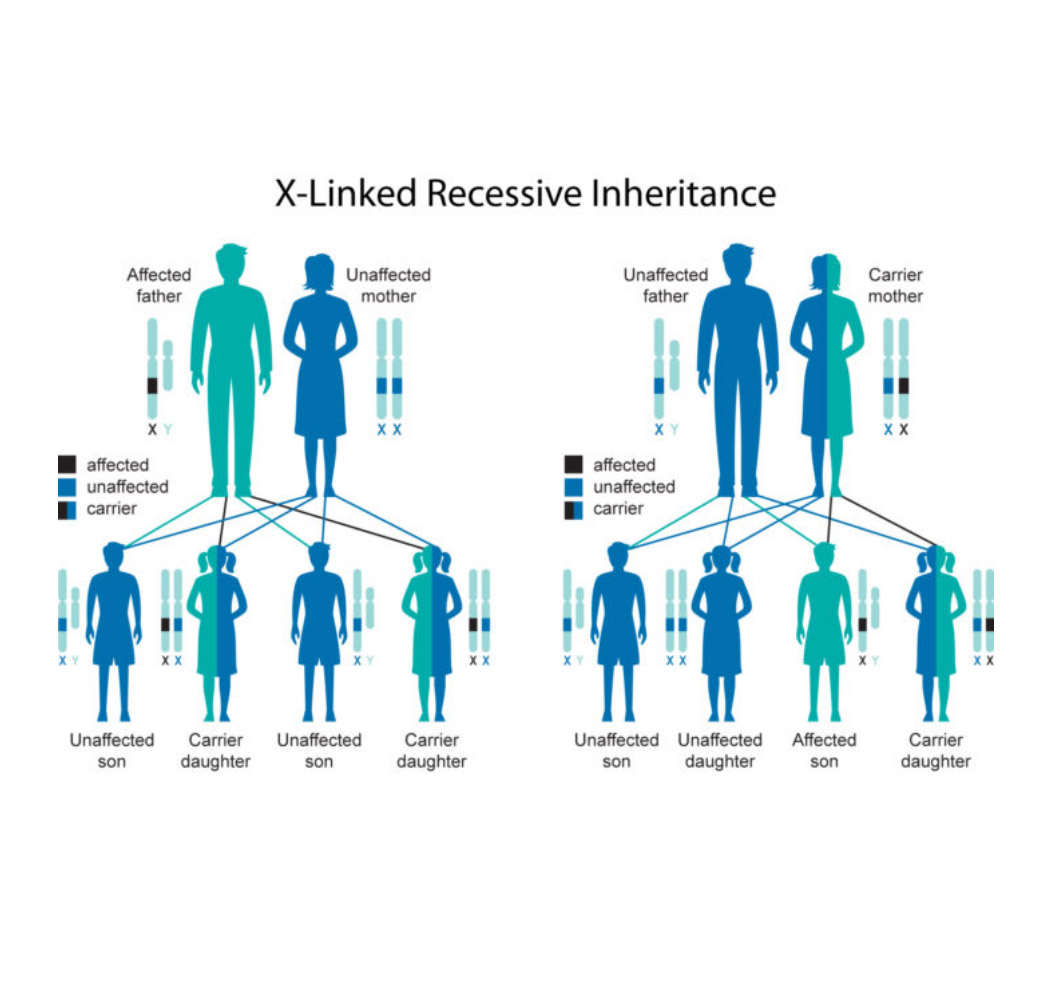
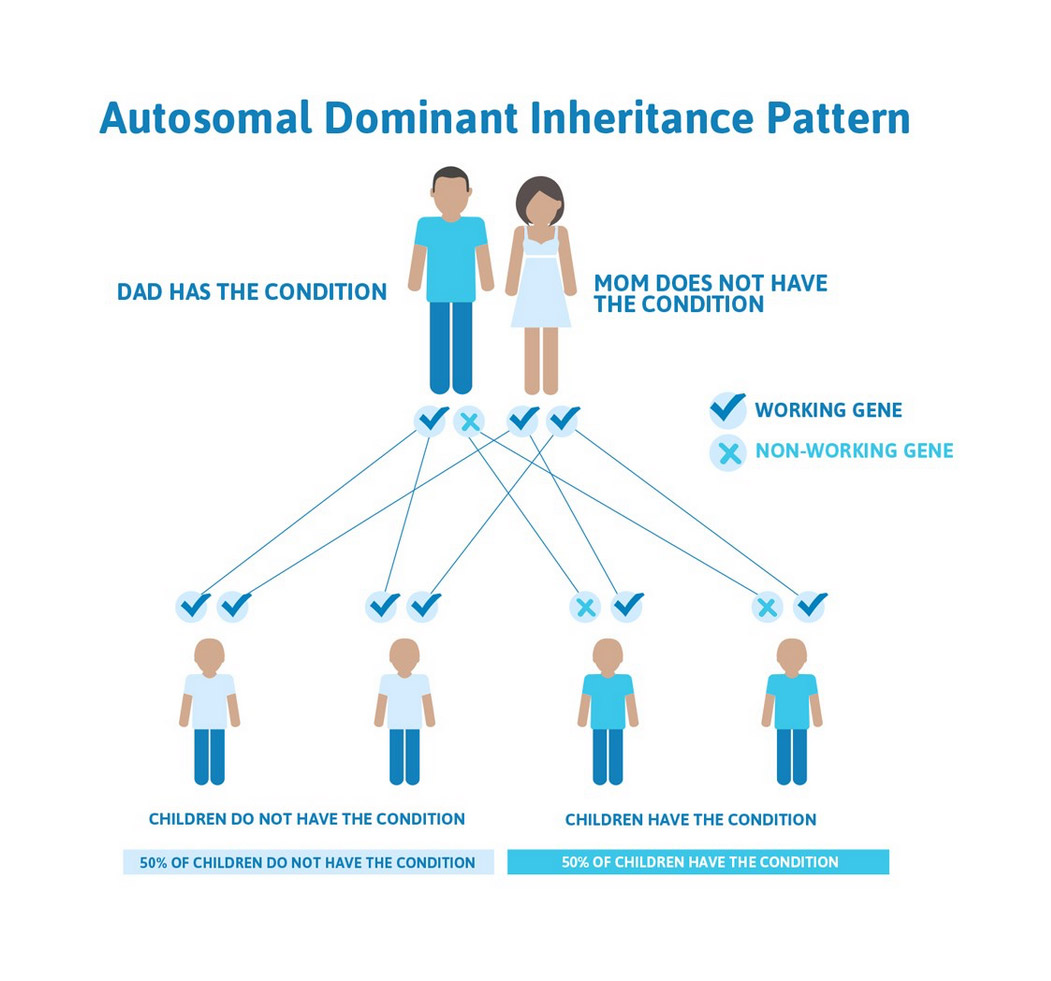
Explaining inheritance
- Instead of: “this condition follows an autosomal dominant inheritance pattern.”
- Plain language dialogue: “This is the kind of condition where having just one copy of a genetic change. Can be enough for it to show up in a person. Each child has the same chance of inheriting it, just like flipping a coin each pregnancy.”
- Optional add-on: “Those chances don’t change based on what happened and past pregnancies.”
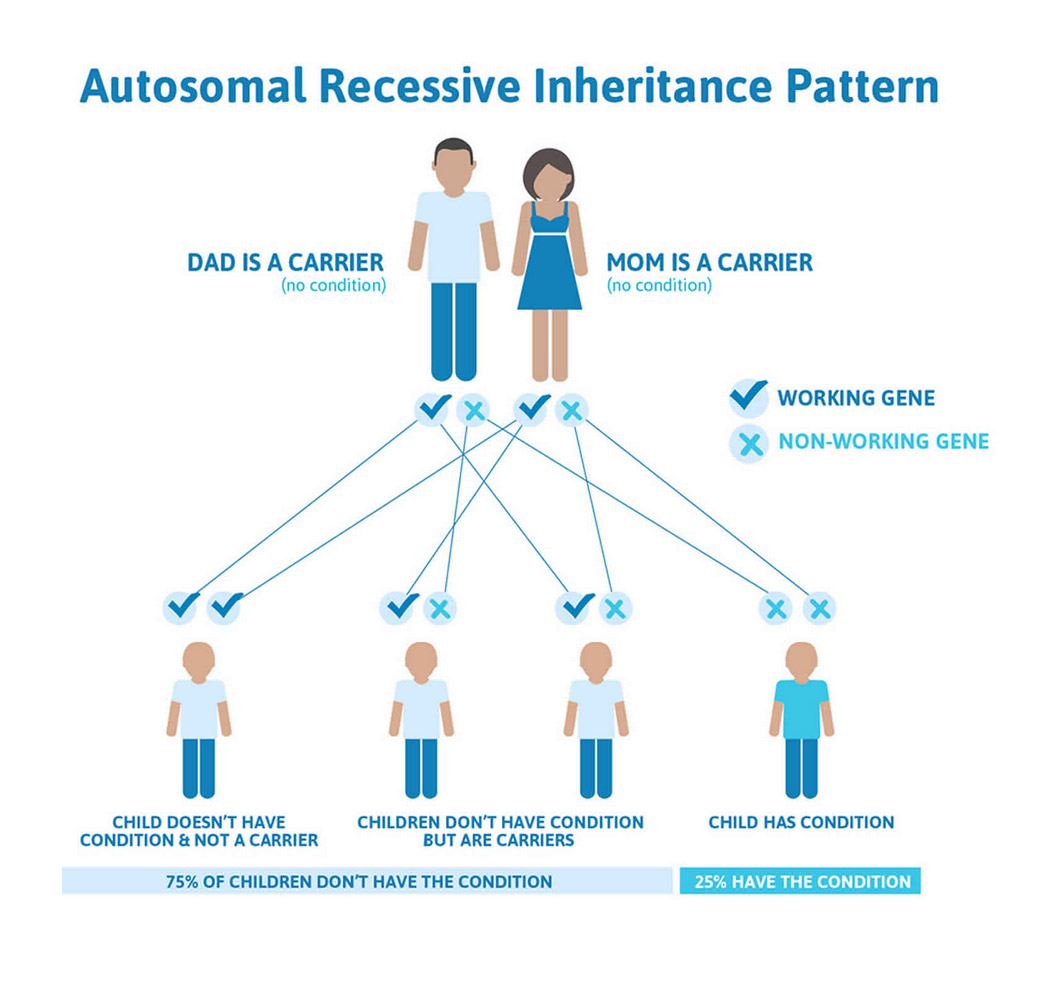
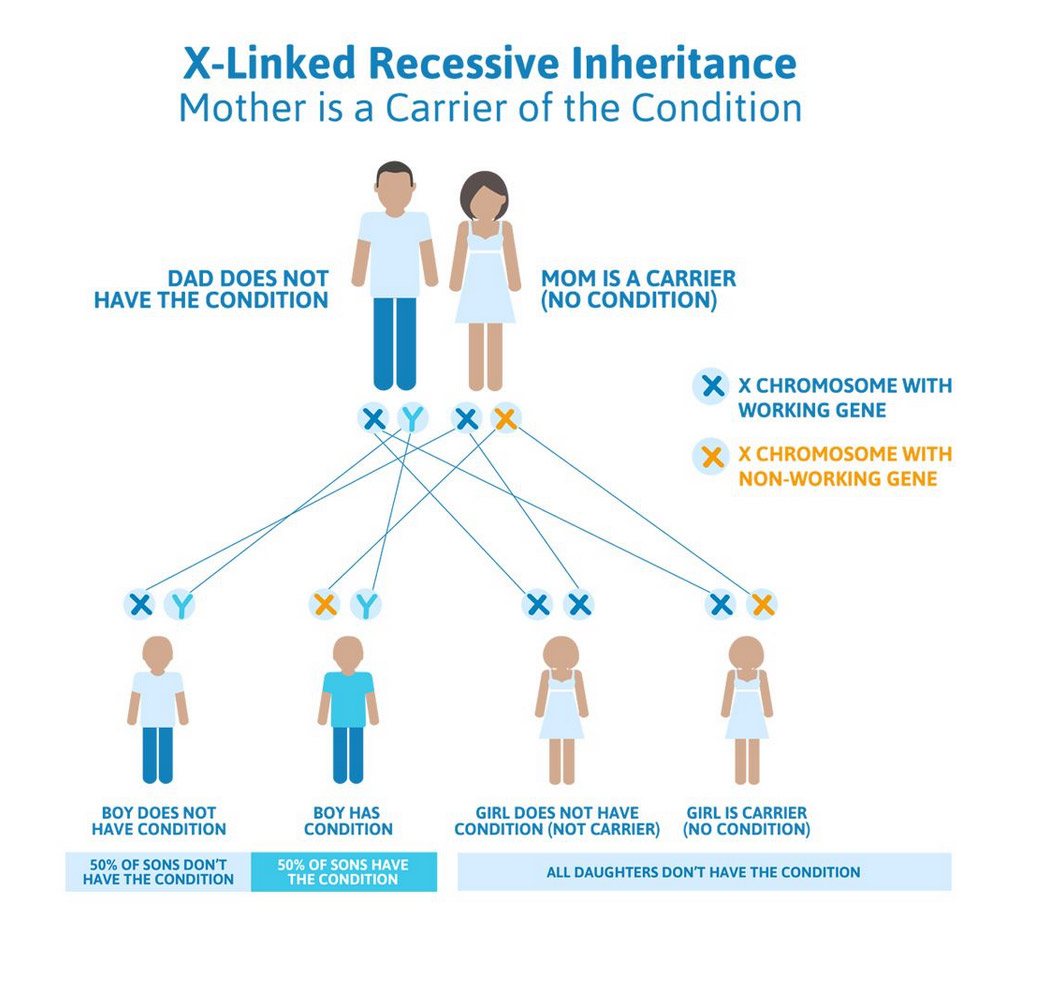
Explaining carrier status
- Instead of: “You’re a carrier but unaffected.”
- Plain language dialogue: “You have one copy of a gene change, but it doesn’t usually affect your own health. It’s something that mostly matters when thinking about future children.”
Explaining genetic testing
- Instead of: “We are ordering a multigene panel to identify pathogenic variants.”
- Plain language dialogue: “Genetic testing looks at certain genes to see if there are changes that help explain what we’re seeing in your health or family history.”
- Optional check-in: “Before we go on, does that match what you were expecting testing to do?”
Explaining uncertain results
- Instead of: “This is a variant of uncertain significance.”
- Plain language dialogue: “This result shows a genetic change, but right now we don’t know if it’s related to health or if it’s just a normal difference between people.”
- Optional to Normalize Uncertainty: “This happens often, and it doesn’t mean anything bad showed up, it just means science doesn’t have the full answer yet.
See more plain language examples
Examples on how to check in for patient understanding
General Understanding
- How is this landing for you so far?
- What questions are coming up right now?
- These normalize pauses and invite reflection without pressure.
Clarity check (frames responsibility on the counselor)
- I want to make sure I explain this clearly, how are you understanding it?
- Is there a different wat it would be helpful for me to explain this?
- Avoid testing the patient; emphasizes shared responsibility.
Teach-back
- Just so I know, I explained this well, how would you describe it in your own words?
- If you were explaining this to someone you trust, what would you say?
- This tool is great during genetics education and testing discussions.
Emotional & cognitive load check
- That was a lot, how are you doing right now?
- Would you like to pause here or keep going?
- Critical when information is complex or emotionally charged.
Learner Skill Practice Activity
Checking for Understanding in Practice: Pediatric vs Adult Cases
Case 1: Adult Genetic Counseling
You’re meeting with a 35-year-old patient referred for genetic counseling due to a family history of a neuromuscular condition. The patient is a wheelchair user and lives with a progressive physical disability that affects mobility and endurance. At the start of the visit, the patient shares that long appointments can be physically tiring, and that they benefit from short examples and clear pacing.
During genetics education about inheritance and testing options, the patient is engaged and asks a few questions or Leon. As the conversation continues, you notice the patient becomes quieter and adjust their position frequently.
Prompt:
- Write one check in question you would use to assess understanding or comfort at this point in the session.
Examples:
- We’ve covered a lot, and I want to check in. How was your energy right now? Would it help to or take a short break?
- Before we keep going, what part of this has felt most clear so far, and what part would you like me to revisit?
- Would it be better to continue talking, or to summarize what we’ve covered?
Case 2: Pediatric genetic counseling
You are meeting with the parents of a six-year-old child who has an intellectual disability and speech differences. The visit is focused on discussing genetic testing options. The child is present in the room, playing quietly with a device. One parent is asking multiple technical questions, while the other appears overwhelmed and is not speaking. The child occasionally looks up when their name is mentioned.
Prompt:
- Write one check in directed toward the caregivers to assess understanding or readiness to continue.
- Write one check in or action that helps keep the child respectfully centered, even if they’re not verbally participating.
Examples:
To caregivers:
- We’ve talked about several possibilities today. What feels most important for you to understand right now?
To center the child:
- Is it okay if I briefly explain this part in a way that includes [child’s name], even if they’re just listening?
- We’ll make sure any next steps take into account what works best for your child now and in the future.
This section also invites counselors to reflect on how societal narratives about disability—explored earlier in the course—may unconsciously shape how testing is presented.
Reflection Prompt for Learners:
Case Example: A couple is referred for preconception genetic counseling. Both individuals have a diagnosis of achondroplasia. They want to know the chances of having a child without the condition versus a child with the condition. When you meet them, they tell you they are very excited to have a child like them.
How could you adjust your language to present genetic testing in a way that is more neutral, values-based, and patient-led? Provide a specific example of dialogue you could use.
6.7 Psychosocial Support
Disability-informed psychosocial support moves beyond crisis intervention to include validation of identity, recognition of resilience, and acknowledgment of systemic challenges. Counselors should be prepared to address emotions related not only to diagnosis or risk, but also to stigma, past healthcare trauma, family conflict, or social exclusion.
Importantly, support should be patient-led. Some individuals may welcome space to discuss identity, advocacy, or lived experience, while others may prefer to focus narrowly on medical information. Asking permission to explore psychosocial topics respects autonomy and avoids over-pathologizing disability.
Case Example
You are providing genetic counseling for a 24-year-old who is deaf and uses ASL as their primary language. They were referred after genetic testing identified a hereditary form of hearing loss. An ASL interpreter is present for the session. The patient shared earlier that they are active in the Deaf community and view deafness as a core part of their identity rather than a medical condition to be fixed. As you review the results, the patient becomes less expressive and briefly shares that previous healthcare and encounters often focused on interventions they did not want. They also mentioned strained family relationships related to pressure to pursue cochlear implantation in childhood.
Prompt: What psychosocial considerations are highlighted within this case?
This case reflects how psychosocial needs may stem not from the disability itself, but from stigma, family conflict, and repeated experiences of being misunderstood and medical settings. The patient’s emotions are shaped by past health care trauma, and by feeling their identity has been minimized.
Instead of assuming distress about the genetic finding, the counselor uses a patient-lead approach:
- People experience genetic results like this in very different ways. Would it feel helpful to talk about how this information connects with your experiences so far or would you rather focus on next steps?
When the patient chooses to share more, the counselor responds by validating identity and resilience:
- It sounds like deafness has been an important part of your community and sense of self, and that some of the hardest parts have come from how others have responded, not from being Deaf itself.”
The counselor avoids reframing deafness as loss or impairment and remains attentive to how family dynamics and past pressure influence. The patient’s current emotional experience. Support is offered without directing the conversation toward intervention or change, allowing the patient to define what support looks like to them.
Reflection Prompts for Learners:
What moments in this case demonstrate validation of identity rather than problem-solving?
What cues indicated when to pause, follow the patient’s lead, or shift focus in this interaction?
Identify one phrase from the case that you would want to practice using in your own counseling sessions. Why that phrase?
6.8 Patient Resources
Providing resources is a tangible way genetic counselors can support equity beyond the session. Disability-informed resource provision includes offering materials in accessible formats and referring to community-based supports, advocacy organizations, peer networks, and disability-specific services—not only medical follow-up.
Counselors should be mindful that access varies by geography, insurance, language, and social identity. When possible, collaboratively identifying resources with patients reinforces agency and relevance.
This step reflects the broader course emphasis on moving beyond medical care toward holistic, community-connected support.
Video: Connecting with Other Parents
A mother reflects on the value of connecting with another parent navigating MPS I, facilitated by her genetic counselor. This narrative highlights how intentional resource sharing and peer connections can provide lasting support beyond the clinic.
Lifespan Care & Follow-Up
Children with medical complex genetic conditions often require care that extends far beyond a single clinic visit or developmental stage. For genetic counselors, providing disability informed care means recognizing that individuals evolve across the lifespan. Lifespan care involves anticipating gaps in services, supporting continuity across specialties, and preparing families for transitions that may bring new challenges. Ongoing follow-up, proactive resource sharing, and coordination with multidisciplinary teams allow genetic counselors to help families navigate uncertainty overtime.
Video: Transitioning from Pediatric to Adult Care: A Parent’s Perspective
A mother reflects on her fear surrounding the transition from pediatric to adult care for her daughter with MPS I. This narrative emphasizes the need for genetic counselors to proactively support families through transition planning and systems navigation.
Reflection Prompt for Learners:
Reflect on how your understanding of disability and disability-informed genetic counseling has evolved throughout this course. How will you apply what you’ve learned to your future clinical practice to promote patient-centered care? Identify at least two specific changes you plan to make in your communication, counseling approach, or clinical decision-making.